

On January 1, 2022, changes to the federal physician self-referral law (“Stark Law” or “Stark”) group practice definition special compensation rule go into effect. Among other things, these changes revise the rule related to overall profits to prohibit pooling and distributing profits from designated health services (“DHS”) on a service-by-service basis, which is sometimes referred to as “split pooling.” As of that date, profits from all the DHS of the practice, or a component of the practice that consists of at least five physicians (a “5+ physician pod”), must be aggregated before distribution. Group practices that use split pooling need to modify their compensation methodologies to account for this change by January 1. Because of the time and effort involved in modifying physician compensation methodologies, now is the time for physician practices to evaluate whether any modifications to their compensation methodologies are needed in order to comply with this change.
Physician practices also need to be aware of important commentary from the Centers for Medicare & Medicaid Services (“CMS”) on the special rule that clarifies CMS’s intentions regarding permissible DHS profit sharing and additional revisions to the regulation text that impact profit sharing, which may also necessitate (or, in some cases, permit) changes to certain group practice compensation methodologies.
These changes and commentary, which are described in detail below, are part of a sweeping set of final rules issued last fall by CMS to revise the Stark regulations, which were part of the “Regulatory Sprint to Coordinated Care” (the “Final Rules”). This white paper summarizes the Final Rules, and more information about the Regulatory Sprint can be found here. Most of the Final Rules went into effect on January 19, 2021, but changes to the group practice definition will not become effective until January 1, 2022. The revised version of the group practice definition that will be in effect as of January 1 is available here, and a redline comparing the version that is currently in effect to the revised version is available here.
Background
Many physician practices rely on the Stark Law’s in-office ancillary services exception to permit their physicians to make internal referrals for DHS. The in-office ancillary services exception generally requires, among other things, that the physician practice qualify as a “group practice” under the Stark Law at 42 C.F.R. § 411.352.
The group practice definition has many detailed and technical requirements. One of the requirements is that no physician who is a member of the group practice may directly or indirectly receive compensation based on the volume or value of their DHS referrals, except as provided in a special rule within the definition related to productivity bonuses and profit shares at 42 C.F.R. § 411.352(i). If specified requirements are met and an exception applies, the practice can take advantage of these special compensation rules, including (among other things) paying physicians a share of the “overall profits” of the practice provided that the share is not determined in any manner that is directly related to the volume or value of DHS referrals by the physician. Under the current regulations, “overall profits” means “the group’s entire profits derived from DHS payable by Medicare or Medicaid or the profits derived from DHS payable by Medicare or Medicaid of any component of the group practice that consists of at least five physicians.” CMS has stated that it believes that a threshold of at least five physicians is likely broad enough to make the ties between compensation and DHS referrals sufficiently attenuated.
Split Pooling Prohibition
In changes to the special rules for payments based on a share of overall profits in the Final Rules, CMS added the words “all the” before “designated health services.” This means that the profits from all the DHS of the practice—or a component of the practice that consists of at least five physicians—must be aggregated before distribution. Thus, under the revised regulations, a physician practice that wants to qualify as a group practice cannot pool and distribute profits from DHS on a service-by-service basis (i.e., “split pooling”).
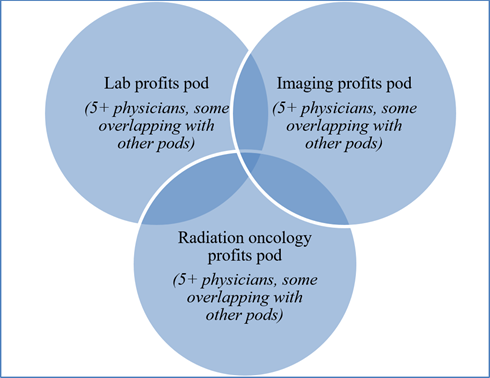
To illustrate, consider a physician practice that has 20 physician owners and/or employees and that provides and bills Medicare for clinical laboratory services, diagnostic imaging services, and radiation oncology services (all of which are DHS) and relies on the in-office ancillary services exception to comply with Stark. This physician practice currently pools and distributes the profits from Medicare-covered lab services to one subset of 5+ physicians; imaging services to another subset of 5+ physicians; and radiation oncology to another subset of 5+ physicians. Some physicians are in more than one of these DHS-specific pods. This is illustrated in Figure 1 below.
Figure 1 – Illustration of split pooling of DHS profits in a physician practice before rule change:
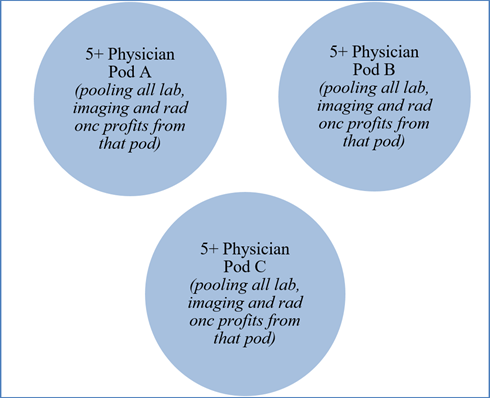
With the change to the group practice definition, if this physician practice wishes to continue to qualify as a group practice, by January 1, 2022 it must modify its physician compensation methodology to no longer use split pooling. It could, for example, aggregate all the DHS profits of the entire group (from lab, imaging, and radiation oncology) at the group level before distribution. Or it could, for example, divide its physicians into multiple 5+ physician pods, and aggregate in each pod all the profits derived from DHS referred by all the physicians in the respective pod before distribution. This means that each of those 5+ physician pods likely has profits from more than one category of DHS, and no physicians participate in more than one pod. This is illustrated in Figure 2 below.
Figure 2 – Illustration of option for DHS profit shares after rule change:
CMS recognized that many physician practices have interpreted the overall profits rule to permit split pooling and that group practices need time to modify their physician compensation methodologies in light of the revised regulations. Further, many group practices establish their compensation methodologies prior to the beginning of each calendar year and an element of the group practice definition essentially requires a group practice’s compensation methodology to be established prospectively. For these reasons, CMS delayed the effective date of revised 42 C.F.R. § 411.352(i) until January 1 of next year.
CMS explained that this regulatory change is a codification of its existing policy, meaning that it reflects how CMS originally intended for the rule to be interpreted. However, CMS did not indicate that group practices currently using the split pooling methodology are violating Stark. But it is clear that as of January 1, 2022, such split pooling will run afoul of the special compensation rules, which would mean the group would not meet the definition of a “group practice” and it generally could not rely on the in-office ancillary services exception. If no other exception applies, all of the practice physicians’ DHS referrals to the practice would be prohibited under the Stark Law. Therefore, it is essential for group practices that currently use the split pooling methodology to modify their physician compensation methodologies by January 1, 2022 to comply with the revised regulations.
Additional Changes and Clarifications Impacting Profit Sharing
CMS made other important comments in the preamble to the Final Rules clarifying its intentions regarding permissible DHS profit sharing and additional revisions to the regulation text that impact profit sharing, which may also necessitate (or, in some cases, permit) changes to certain group practice compensation methodologies. These included:
- Distribution methodologies:
- CMS confirmed that a group practice may utilize different distribution methodologies to distribute shares of overall profits from all the DHS of each of its 5+ physician pods (for example, per capita or based on personal productivity). But a group practice has to utilize the same methodology for distributing overall profits for every physician within a single component.
- Accordingly, using the illustration shown in Figure 2 above, the practice could distribute shares of overall profits from all the DHS of Pod A on a per capita basis; of Pod B based on personal productivity; and of Pod C using a per capita basis, productivity basis, or some other basis that is not directly related to the volume or value of the Pod C physicians’ referrals. However, the practice would have to use the per capita methodology for every physician in Pod A, the personal productivity methodology for every physician in Pod B, and the methodology chosen for Pod C for every physician in Pod C. It could not use different methodologies to distribute the profits of different types of DHS within each of the pods.
- If there are fewer than five physicians in a group, “overall profits” mean the profits derived from all the DHS of the entire group. Here, the group may aggregate DHS profits among less than five physicians, because the entire group is less than five physicians.
- CMS confirmed that any physician in the practice may be paid a share of overall profits of the group practice; the share does not have to be just among owners.
- Nothing requires a group practice to distribute DHS profits to physicians. But if the group is paying a share of overall profits from DHS, it must first aggregate all profits from the entire group or a 5+ physician pod (as described above). Once overall profits are aggregated, the group may retain some of the profits or distribute all of them through shares of overall profits to physicians.
- Nothing prohibits using eligibility standards to determine whether a physician is eligible for a profit share (e.g., ownership status, longevity, full vs. part-time employment status), but the standards cannot result in payment of a share that is determined in a manner that is directly related to the volume or value of a physician’s referrals.
- A group can establish its 5+ physician pods by including in each pod, for example, physicians at the same practice location or physicians with similar practice patterns, years of experience or longevity, or other criteria the group determines, again as long as the share of overall profits received by a physician is not determined in any manner that is directly related to the volume or value of the physician’s DHS referrals.
- CMS included some important reminders in the Final Rules for group practices that establish 5+ physician pods for DHS profit sharing. While it is permissible to have location and specialty-based compensation practices with respect to revenues derived from DHS if the requirements at 42 C.F.R. § 411.352(i) are met, the group must ensure that doing so does not compromise its compliance with other elements of the group practice definition, including:
- The “unified business” test, which requires the group to be a unified business having at least the following features: (i) centralized decision-making by a body representative of the group practice that maintains effective control over the group’s assets and liabilities (including, but not limited to, budgets, compensation, and salaries); and (ii) consolidated billing, accounting, and financial reporting. CMS explains that group practices cannot be “loose confederations of physicians that are group practices in name, but not operation.” It is important that groupings of 5+ physician pods do not indicate a lack of a unified business, or a business that is unified only regarding capturing the profits from DHS referrals. The group needs to think of the “group practice” as the practice at an entity level, and the 5+ physician pods as components of that entity.
- The “substantially all” test, which requires (among other things) that revenues from patient care services are treated as receipts of the group. So, the group must ensure that such revenues are treated as receipts of the practice as a whole (i.e., rather than receipts of the 5+ physician pod).
- CMS revised two of the deeming provisions of the overall profits rule to use the term “overall profits” to clearly articulate that these deeming provisions relate to methods for distributing a share of the overall profits, not “profits” (i.e., revenues minus expenses) or “revenues” (i.e., without expenses deducted). CMS explained: “Although it may be true that it is easier to calculate revenues than to calculate profits, in general, we believe that a group practice’s distribution of revenues to a referring physician rather than profits, which are calculated by deducting the expenses incurred in furnishing the designated health service, could serve as an inducement to make additional and potentially inappropriate referrals to the group practice.” Thus, when using these deeming provisions, a practice needs to make sure that it is using profits rather than revenues.
- As described above, the definition of “overall profits” currently references profits from DHS payable by Medicaid, and CMS removed the reference to Medicaid in the Final Rules. CMS confirmed that the definition of DHS at 42 C.F.R. § 411.351 includes only DHS payable in whole or in part by Medicare, so “DHS payable by Medicaid” would not include any services. For the same reason, CMS changed the special compensation rule deeming provisions that stated “. . . are not DHS payable by any Federal health care program or private payer” to “. . . are not DHS and would not be considered DHS if they were payable by Medicare.”
Finally, CMS made changes and clarifications in the Final Rules that apply beyond profit sharing, but that may impact the way that a group evaluates and structures its profit sharing. As described in more detail in this white paper, these include:
- As of January 1, 2022, profits from DHS that are directly attributable to a physician’s participation in a “value-based enterprise” (as defined in the Stark regulations) can be distributed directly to the participating physician, without having to aggregate the profits with the overall profits of the group or a 5+ physician pod.
- A new special rule regarding compensation that takes into account the volume or value of referrals at 42 C.F.R. § 411.354(d)(5) and (6) applies with respect to the volume/value standard and the special compensation rules under the group practice definition. Thus, it is important for group practices to understand the new volume/value rule.
Conclusion
As stated above, it is not too early for group practices to evaluate whether any changes are necessary to their physician compensation methodologies in order to comply with the prohibition on split pooling of DHS going into effect on January 1, 2022, as well as to evaluate whether any other changes are necessary to their group practice structure and operations in light of revisions and clarifications made in the Final Rules. If you have any questions about compliance with the group practice definition, please contact the authors or any member of Dorsey & Whitney’s Healthcare Transactions and Regulations Practice Group.